Brain tumors remain a significant health problem in the worldwide. Overall, they comprise some of the most malignant tumors known to affect human beings and are generally refractory to all modalities of treatment.
Angiogenesis underlies all tumor growth by providing oxygen and nutrients to support increased cellular proliferation and metabolism and to remove waste products. However, tumors cannot create their own blood supply and when malignant tumors are very small, they rely principally on diffusion for survival. If a tumor is to grow beyond a few millimeters in size, angiogenesis will be required. In the central nervous system, gliomas are most studied tumors with regard to MR perfusion imaging. In the treatment of brain tumors, surgical intervention remains a common and effective therapeutic option. Recent advances in neuroimaging have provided neurosurgeons with new tools to overcome the challenge of differentiating healthy tissue from tumor-infiltrated tissue, with the aim of increasing the likelihood of maximizing the extent of resection volume while minimizing injury to functionally important regions.
What kind of doctor does brain imaging? Brain imaging helps neurosurgeons diagnose, treat, and monitor people with an array of neurologic issues.

Modalities
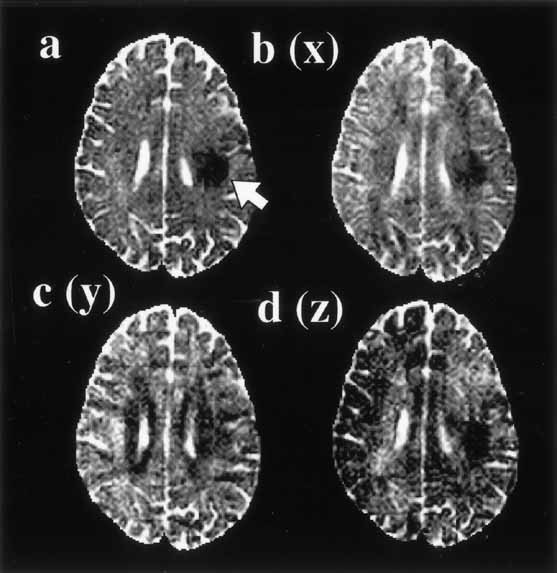
- Diffusion
- DTI
- IVIM
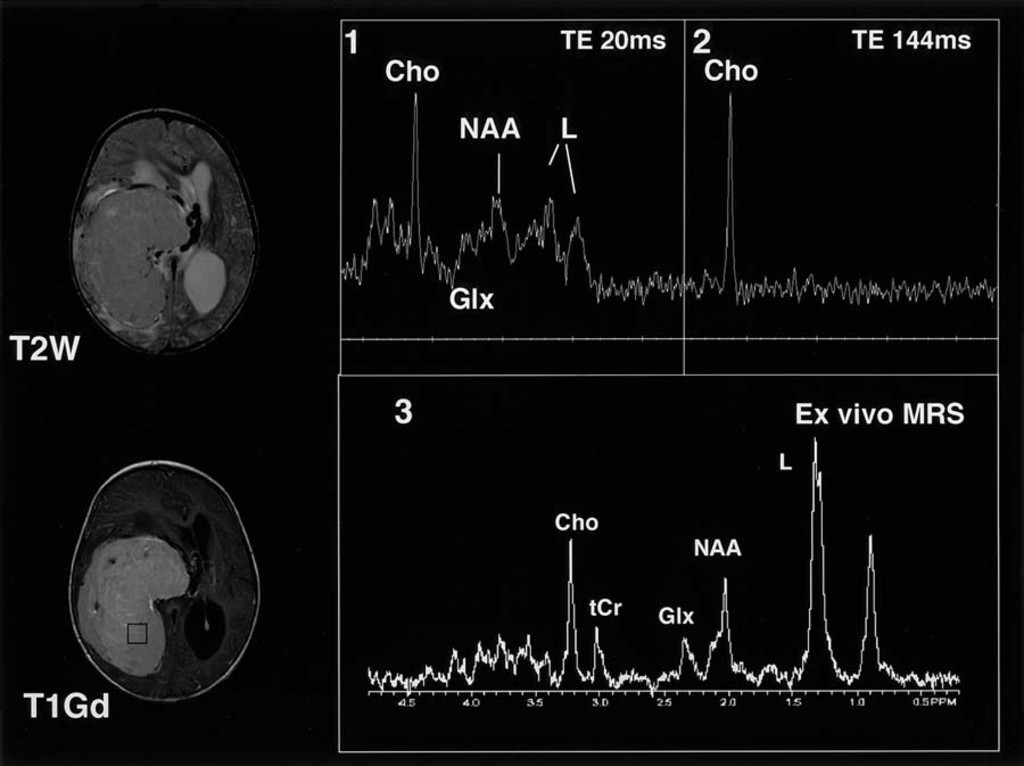
- MRS
- DSC
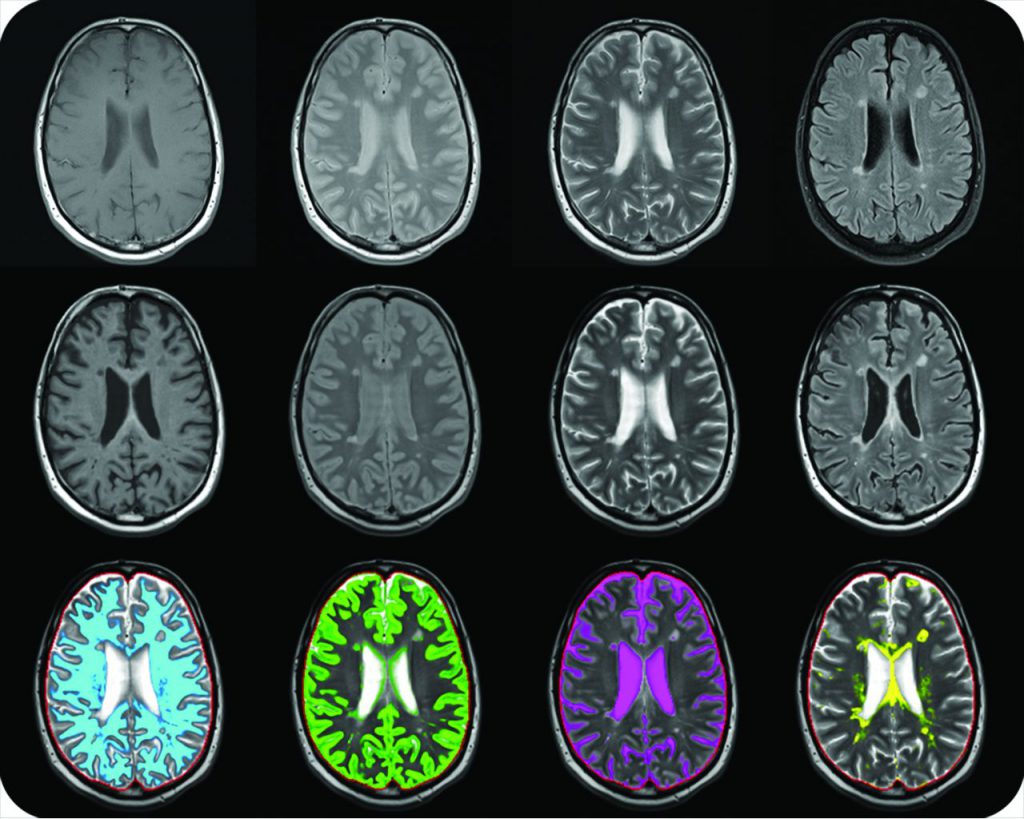
- T1
- T2
- Proton Density imaging
How AI is improving cancer diagnostics? In people with only one scan available, the AI outperformed all of the six radiologists who also examined the CT scans to assess risk of lung cancer. The AI reduced the number of false positives by 11% and false negative by 5%. When there were two scans, the radiologists did about as well as the computer.
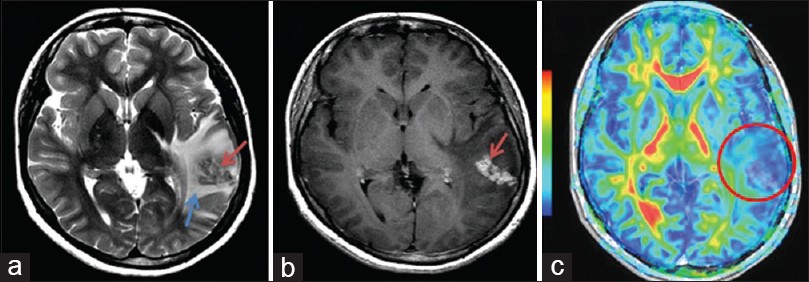
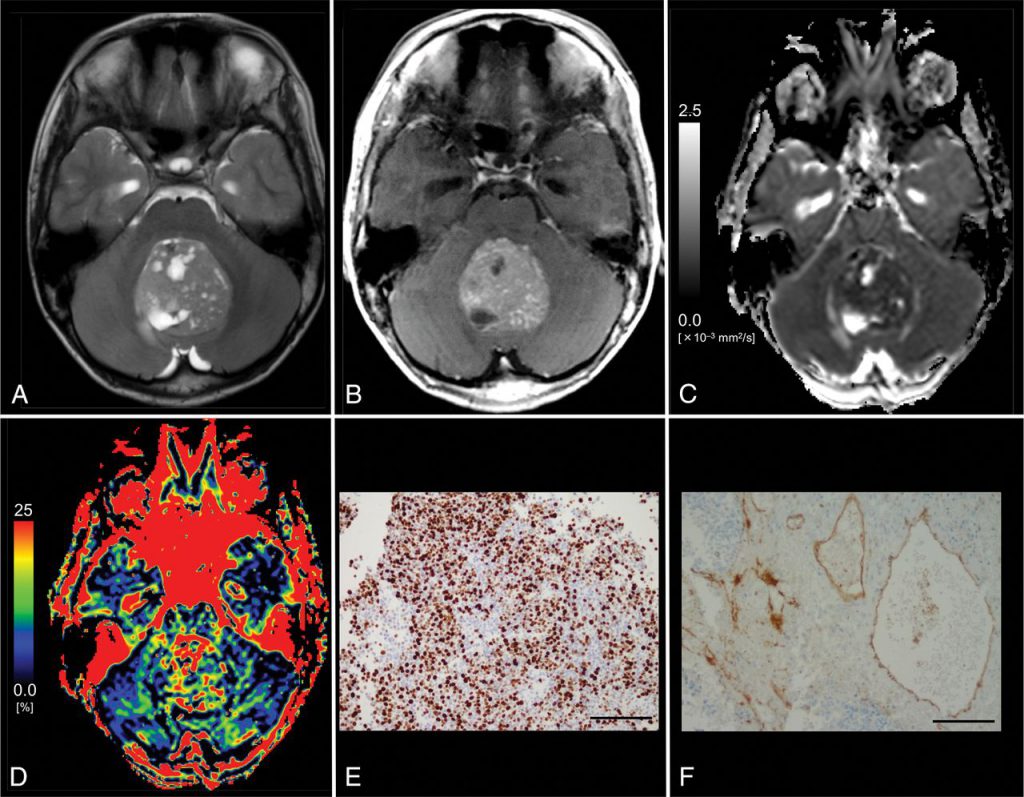
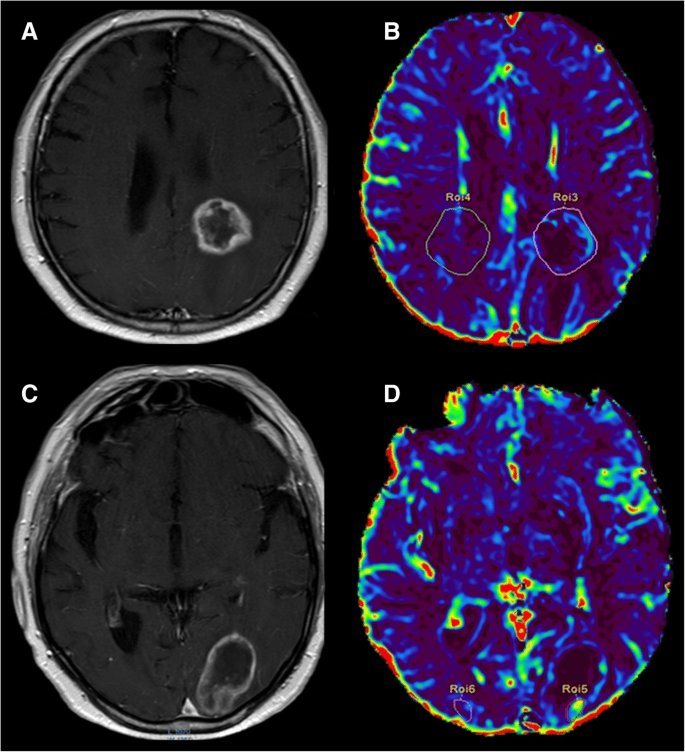
DSC
DSC-MRI measurements of tumor rCBV have been widely used in neuro-oncology for glioma grading, prognosis prediction and differentiating recurrent
tumor from radiation necrosis. Although the WHO classification remains the gold standard for prognosis and treatment in brain tumors, DSC-MRI can help predict glioma grade and therefore better direct therapy. DSC-MRI can also help locally guide biopsy and treatment based on the portion of the tumor that appears the most aggressive, which is not necessarily the part of the tumor that most avidly enhances. DSC imaging may be able to predict time to progression in patients with glioblastoma.
What is brain perfusion CT scan? Computed tomography (CT) perfusion of the head uses special x-ray equipment to show which areas of the brain are adequately supplied with blood (perfused) and provides detailed information about blood flow to the brain. CT perfusion is fast, painless, noninvasive and accurate.
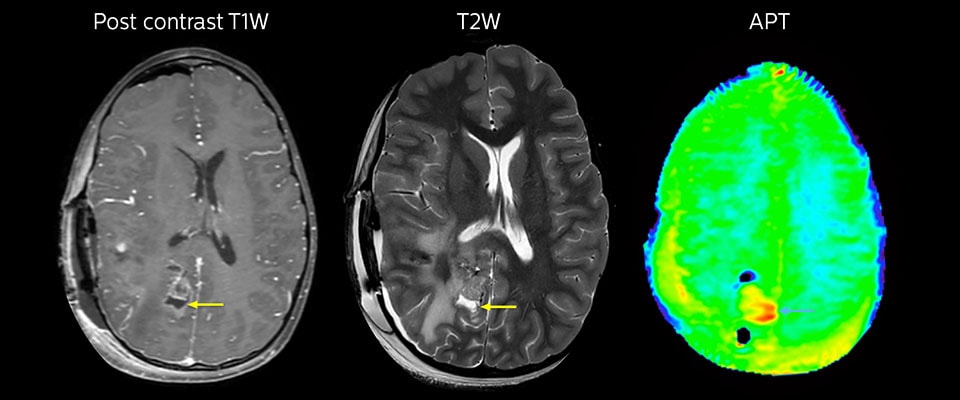
T1
Using the absolute T1 values in the brain before and after intravenous injection of contrast agent, a measurement of contrast agent concentration per voxel of the tumor can be calculated. Dynamic imaging of T1 relaxation time during contrast agent injection can be used to objectively locate these xenograft brain tumors and to track gadolinium-based contrast uptake over time.
The T1 parametric maps made it easy to identify the regions of contrast enhancement and thus tumor location. Doubling the typical human dose of contrast agent resulted in a clearer demarcation of these tumors. Therefore, T1 imaging of brain tumors is gadolinium dose dependent and improves detection of tumors by MRI. The use of T1 maps provides a quantitative means to evaluate tumor detection by gadolinium-based contrast agents over time. This dynamic quantitative T1 imaging technique will also enable future quantitative evaluation of various targeted MRI contrast agents.
What does T1 mean in MRI? T1 (longitudinal relaxation time) is the time constant which determines the rate at which excited protons return to equilibrium. It is a measure of the time taken for spinning protons to realign with the external magnetic field.